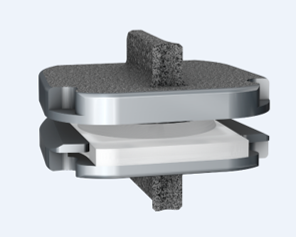
By now you’ve heard a lot about artificial discs, or disc arthroplasty, as a treatment for certain kinds of neck problems including cervical disc herniation or cervical disc degeneration.If you’re looking for scientific papers on the subject, you can find over 150 peer-reviewed publications on Pub-Med or in the Scientific and Medical Journals that focus on surgical treatment. But what if you just want to know what they look like and how they work? Well, let’s break it down! What is an artificial disc? An artificial disc is used to replace the damaged intervertebral disc that is removed during discectomy as treatment for a disc herniation or disc degeneration.  Placement of the artificial disc, more commonly referred to as a disc arthroplasty or cervical disc replacement, fills the gap left when the original disc is taken out. In so doing the artificial disc restores the original, normal disc height, holds the adjoining vertebra in normal alignment, and preserves a small amount of motion in flexion and extension, side to side rotation, and left and right side-bending – about the amount the normal disc had when it was healthy. A spinal fusion – the traditional solution after discectomy – can do those first two things very well, but it eliminates all motion at that level, leaving the rest of the spine to take up the slack. How does the disc replacement work? The disc replacement device, or implant, is designed to insert into the disc space – the gap left after the disc has been taken out – with minimal removal of normal bone or ligament tissues, and is held in place with small teeth that grab the bone, and with the normal tension of the remaining soft tissues holding it firm. 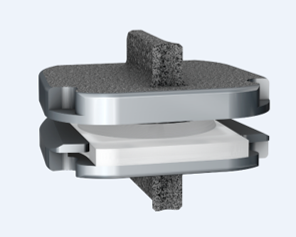 The bone of the vertebrae will eventually grow directly into the top and bottom plates of the device making the fixation permanent, but right from the start the fit of the specific disc designs is such that loosening or slippage of the device is very rare, even with early motion and activity. So, they don’t need to be screwed in or cemented into place, and you don’t need to wear a hard collar or immobilizer while recovering from surgery. How are disc replacement implants designed? There have been many different designs of artificial discs created over the last 40 years, and a lot of different materials have been tried from one time or another. Spine surgeons have benefited A LOT from the much longer and sometimes fraught experience of our total joint colleagues who have been studying these issues for many decades longer. The implant designs that I use now are all FDA approved, studied in numerous scientific trials, and have been in use around the world for at least a decade in each case, and much longer in some cases. The primary design for each of the implants I use is the same: Each disc design has three parts: two metal plates – one top and one bottom - and a plastic insert or spacer in the middle. 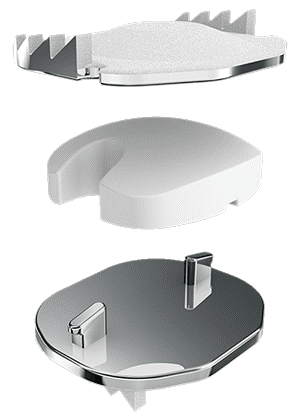 The plates are made of a mix of metals commonly used in spine and joint replacement surgery (cobalt, chromium, and molybdenum in some cases, and titanium in others). The plates typically have either teeth on the top and bottom that help hold the plates to the vertebrae, or small thin “keels” that slot into the bone above and below. The teeth or keels are pressed into the bone without any bone removal, which makes the implant designs I use easy to place properly, without cutting away normal bone. The surfaces of the top and bottom metal plates are typically sprayed with a coating of a bone forming material (hydroxyapatite) that stimulates the vertebral bone to grow and attach to the metal plates for long term stability. The plastic insert that fills the space between the plates differs from implant to implant. In most implants the insert is made from a high molecular weight polyethylene, a material with enough density to resist wear and deformation over time, but “slick” enough to provide very little friction as it slides back and forth against the upper and lower plates. This is the same strategy and material used in our most successful and long-lasting hip and knee replacements. The insert is designed to move a little back and forth and side to side as you move your neck, mimicking your natural joint motion. How big is the implant? They come in different sizes, in order to properly fit different size patients. (Interestingly, your body size does not necessarily tell me much about the size of your spinal elements: some very big people have a surprisingly small bone structure, and vice versa!).  Typically, though, the implant is not much bigger than the size of your thumbnail, and not taller than two or three quarters stacked together. The four disc replacement implants I current use are all FDA approved and well-studied across the globe. Full disclosure – I have been asked to teach surgical techniques to other surgeons from time to time, and I do participate in Investigational trials for some implants ( I was a Principle Investigator for the original MobiC two-level FDA study 15 years ago, and am an investigator for Centinel Spine’s two-level Investigational Device study now), but I am not a paid consultant for any of these companies. So, I can honestly say I pick the implant that suits my patient’s situation best, each time!  MobiC – ZimVie is a new name for a long-established company, and the most widely used two-level implant in the US. You can learn more about their implants here. 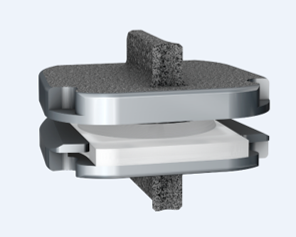 Pro-Disc-C – One of the first to bring an artificial disc to the lumbar spine world, they have a long-established and successful product for single level surgery, and Centinel Spine is sponsoring an ongoing investigational study for their new implants for two-level surgery.  M6 – Provided by Orthofix, this implant has a unique central core that also provides a little more cushion, in theory, than the solid high molecular weight polyethylene cores, and fits certain disc configurations very well.  Simplify – A newer entry provided by Nuvasive, this implant has titanium plates top and bottom, which eliminates any concern for those with metal allergies, and is approved for two level use.
Thanks for reading! I hope you found this both interesting and informative. Feel free to Like and Share this content and please comment to let me know what other questions you might have!
1 Comment
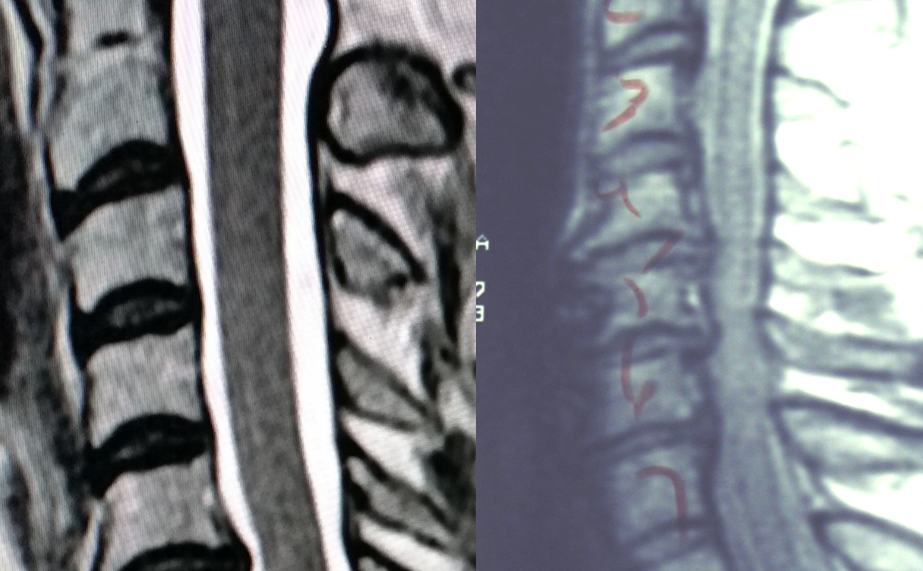
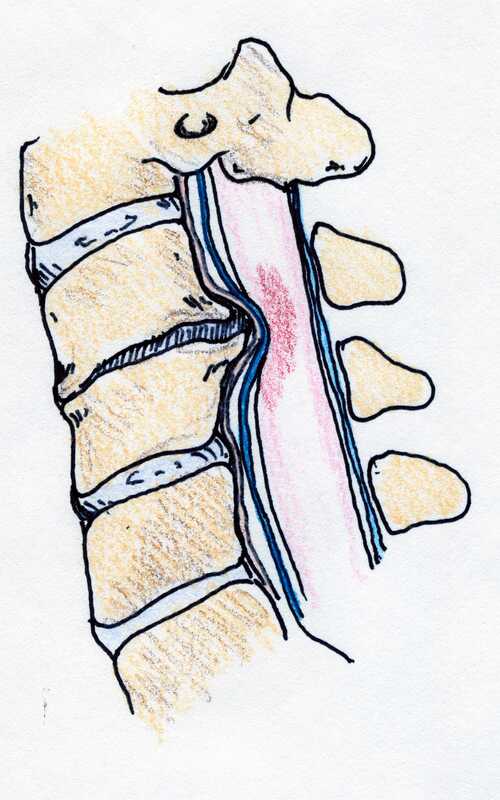
Cervical Disc Arthroplasty: Motion preservation for patients with severe neck pain and arm pain due to disc herniation or degenerative disc disease. Disc replacement surgery represents a powerful, well-established tool for treating disc herniations and cervical disc disease in selected patients. That’s good news for patients who have persistent pain and dysfunction due to neck pain, who still want to avoid a spine fusion if they can. So, what’s the role of Disc Replacement Surgery in 2022? There’s good news and bad news…  Good news!! Most patients with neck pain recover without surgery: 80-90% will get better, and back to normal activity with physical therapy, anti-inflammatory meds, rest, activity modifications, chiropractic manipulation…or, in some cases with nothing but time and TLC! Bad News!! About 10-15% of patients with a serious neck problem will eventually need surgery. They’ll need an operation to relieve persistent arm pain due to a herniated disc, arm pain and weakness due to nerve root compression caused by disc degeneration, or surgery to treat instability or deformity. When persistent neck and arm pain are annoying, we can treat those well with a number of different non-operative strategies – physical therapy, manipulation, oral medications, or injection therapy. But when pain is bad enough that it interferes with daily function, employment, fitness, sleep…surgery starts to make sense. Who needs spine surgery? We consider surgery for patients who have structural neck pain problems, such as disc degeneration, instability, deformity or more serious issues such as fracture, infection, or tumor. We also depend on surgery as a reliable solution for many causes of arm pain or weakness (radiculopathy) including disc herniation, cervical stenosis, or segmental instability.  Not every type of operation works for each of these problems, though, and each has its strengths and its drawbacks. Disc replacement surgery is an excellent treatment for disc herniations and disc degeneration, but it is not a treatment for spinal instability or deformity, and not at all useful for treating tumors, infections, or fractures and dislocations of the cervical spine. Cervical fusion remains the very best solution for each of those problems. For those patients who suffer neck and arm pain due to disc degeneration or herniation, disc replacement – or cervical arthroplasty – is an important option.  Who needs disc surgery? Degeneration of the Intervertebral Disc causes changes in disc, which sits between each of the vertebral bodies and acts as a shock absorber and slightly flexible joint. As we age, the molecular components of the disc change, resulting in a loss of water-holding capacity, and a progressive loss of elasticity and compressive strength – the disc becomes a less successful shock-absorber. On x-rays we see: Bone spurs (osteophytes) form around the facet joints and edges of the discs themselves Disc damage that causes bulging and herniation Loss of normal mechanical stability, loss of disc height, and loss of normal neck posture We can even see structural deformity These changes go along with the symptoms we see: Axial neck pain – pain in the muscles and ligaments of the neck, stiffness, shoulder and back pain; Referred pain - symptoms over the trapezius, rhomboids, and shoulder blades Tension myositis - muscular pain, often causing headaches; and Radicular pain - pain in the spinal nerve distribution causing pain down the arm and into the hand and fingers Radicular arm pain is the symptom most commonly requiring surgery. When these symptoms are severe, interfering with fitness health, and normal rest, and when they fail to improve after a good trial of non-operative care, that’s when we consider surgery. The general rules for choosing surgery for a patient start with the symptoms:
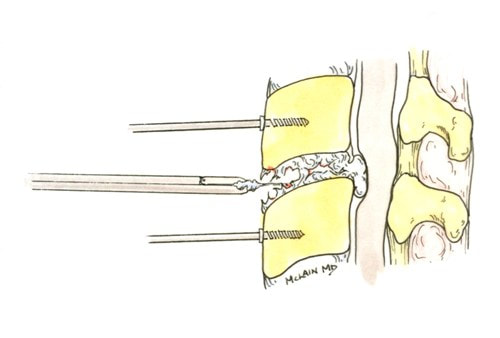 The traditional treatment for cervical disc herniation is an anterior cervical discectomy (surgical removal of the disc) and fusion (ACDF). That’s a surgery through the front of the neck, through which the disc is removed all the way back to the spinal canal. But, why fuse the spine after you get the disc out? The interbody fusion (placing a cage or bone between the endplates of the adjacent vertebrae) restores intervertebral and foraminal height, immobilizes the painful segment, and provides permanent stability. But it eliminates motion at the treated level and increases stresses in the adjacent levels above or below, and that can lead to breakdown at that adjacent level, (adjacent level degeneration) sometimes just a year or two after the initial surgery. What does the Artificial Disc do that’s different? The cervical disc arthroplasty or disc replacement is intended for the patient who would otherwise need a fusion.  The approach for the disc arthroplasty, and the removal of the damaged or herniated disc is exactly the same as in the traditional ACDF procedure, but instead of placing bone or a fusion cage in the empty disc space, disc replacement surgery replaces the damaged intervertebral disc with an artificial device that restores disc height and alignment and preserves the motion of the original disc. This allows the treated spinal level to move more naturally, reducing the risk of adjacent level degeneration down the road. Who is a good candidate for a disc replacement?
 Where will disc arthroplasty work well?
Success has been unequivocally demonstrated in the well-maintained but painful disc, in the young and active patients. What about older patients? If patients are reasonably fit, and bone quality is good, age isn’t a big factor! Studies of disc replacement have included patients up to age 69, and my experience with patients older than this suggests disc replacements are just as successful, and better tolerated than the traditional fusion. What about activity level? Patients that are athletic or hard working can depend on disc replacements to hold up to high demands – they are not fragile. What about smokers? Well, first off – stop! It’s not good for you. However, smoking does not affect the outcome of disc replacement surgery the way it can a fusion, so disc replacement is probably a better choice for you too. Here's the caveat:
With that in mind, cervical disc arthroplasty offers an attractive and valuable option for most patients otherwise indicated for cervical fusion to treat their neck and arm pain. If you’ve been offered a fusion surgery, ask your surgeon if you’re a candidate for disc replacement! As always, I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share this content with others that might find it beneficial! Any good medical exam starts with a careful history. That means answering some important questions, so be prepared!Back and neck pain are common problems that most all of us will experience at one time or another. However, the cause of each person’s pain and the way it affects their life and function can differ significantly. One of the most common causes of failed spine surgery and failed back care is failure to make the correct diagnosis up front, and the subsequent failure to provide the best treatment thereafter – doing a surgical procedure that wasn’t helpful or failing to operate when someone really did need it. One of our most important tools in medical diagnosis – of any kind – is called the “History”. Without a good history, we tend to make assumptions, and if they are the wrong assumptions then we can start down the wrong path when it comes to treatment. That can lead to delays in recovery, unnecessary procedures, or a poor outcome all together. No one wants that!  So, your doctor will want a full and accurate history to help them understand what your particular problem is and how it affects you, so they can provide you the very best and most specific care. Here are Six Questions you should be able to answer for your Back Doctor when you come to talk about back and neck pain or back and neck surgery: 1. What can I do for you today? “Just fix me” sounds cute, but it’s not a helpful answer. Tell me what brings you in today – “I’ve had back pain for years, but for the last 3 – 6 months I’ve been getting terrible leg pain and it worries me” or “ I’ve been diagnosed with a neck strain, but it’s not getting better and my doctor thinks I need to see a specialist”. It’s OK to say “I’m not interested in surgery, I just want to make sure it’s not something serious!”. 2. Where does it hurt? – Sounds simple enough, but every day I meet patients who said “neck pain” on their intake form yet immediately describe burning pain running down their arm to their hand as their real problem. This is important information and it’s important to be thoughtful and specific in your description. And, if the answer changes with activity or time of day that’s important too. “When I first get up my pain is right in the middle of my back – low down, but after I’ve been up and standing, it starts to run down the back of my legs to my feet and toes. Is that weird?” No – it’s important information. 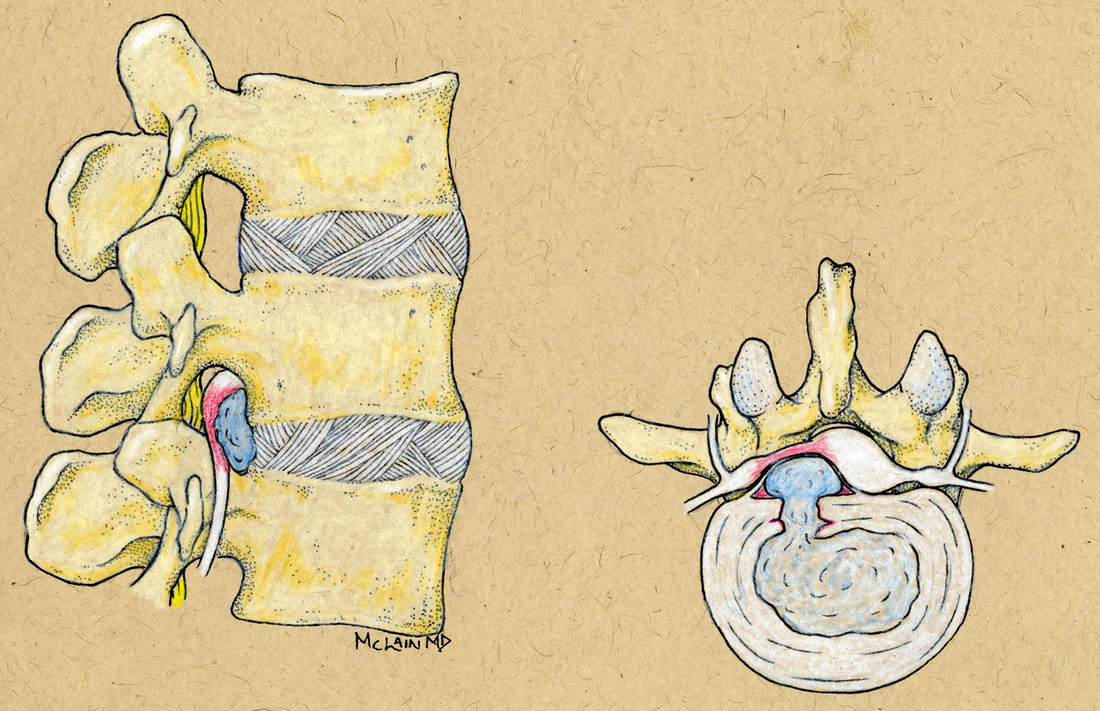 3. How bad is your pain? This is always a hard question to answer, because we each experience pain in different ways at different times. The best way to measure pain is sometimes in terms of what it prevents us from doing. If the pain is severe enough that it’s interfering with your ability to sleep, exercise, and/or work, that’s important. If non-operative treatments don’t get you significant relief, surgery might be a serious consideration. If it’s keeping you from enjoying more than three or four rounds of golf each week, that’s important too, but it suggests you’re functioning pretty well, and a sports/rehab approach might be right for you! 4. How long have you been having pain? It’s important to be clear – I recently had a long conversation with a patient who reported that her pain had started “about three weeks ago”. After looking through the patient’s records I asked why they had had previous x-rays and MRI studies. “Oh, I’ve had back pain for years. But this time it’s been going on for three weeks”. It’s okay to be a little more detailed – “I’ve had back pain for years, but the leg pain didn’t start until the last six months, and it was just last month that it became severe and the numbness and tingling started”. 5. What have you been doing to treat the pain? Your doctor will want to know, and your insurance provider – Medicare, Medicaid, or any other – will quite literally tick off the boxes on previous treatments before they approve any surgery, injection therapy, or even an MRI. “I take an anti-inflammatory medication regularly, with some benefit. I’ve had a complete course of physical therapy, starting in…and ending in…(know the dates), and it didn’t help me much”, or “I tried to do physical therapy, in …(know the dates), but it made my pain worse and I had to stop”. If you’ve had injections or other treatment, make a note of when that was, where it was, and who your doctor was. “I’ve had injections recently, but they didn’t help or at least not very long. They were done by Dr. …, and they were epidural injections/selective nerve root blocks/trigger point injections/facet blocks…”. If you’ve had a previous operation, who did it and what did they do? Bring records with you when you can. When insurance companies deny treatments or demand an appeal for treatment, it’s usually based on lack of previous treatment or lack of documentation of previous treatment. 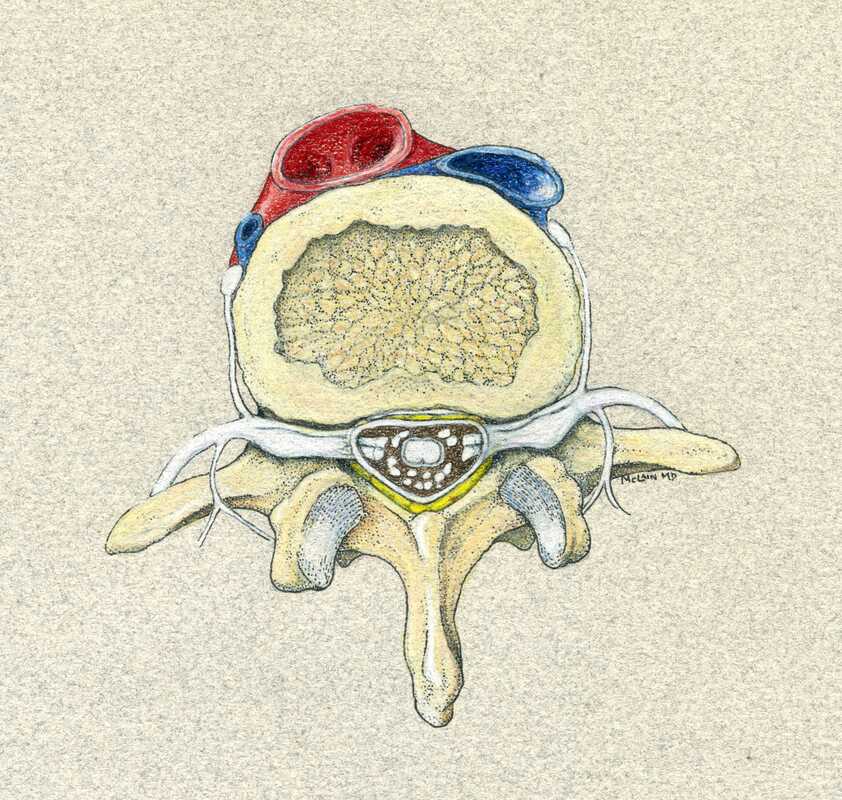 6. Are you working at your regular job right now? This isn’t just a question about your insurance, but one about how your pain is disrupting your life. “I am not working at my regular job, which involves a lot of bending, lifting, or twisting, but my company is great and they’ve got me a light duty job that’s easier to do” is a completely different answer and situation from “ my boss hates me and says I can’t come back unless I can go back to the loading dock”.
But it’s just as important to know that, if you work in the home, you can’t carry a load of laundry, pick up your children or do your household tasks. In either case it’s appropriate to ask the question: Do you need a back operation, or do you need a better job or more help in the home? Making a correct diagnosis and putting together a sound treatment plan depends on understanding where your pain is coming from, how it’s affecting your life and impairing your function, and understanding whether it’s likely to respond to a program of non-operative treatments and therapy or whether there is likely to be a need for surgery. So don't get frustrated with all the questions - it's your chance to guide your doctors in the right direction. If you can provide a clear and accurate History for your doctors, its much more likely that you’ll get the care you need, when you need it, with the best possible outcome. Thanks for reading! Feel free to Like and Share this content and let me know what other questions you might have! Five (OK TEN) things no back patient should ever do…how many are you guilty of?
 So, please be careful…I want you to be active, but take care of your back and use good common sense!
I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share this content with others that might find it beneficial! If you’ve been to more than one doctor for a neck pain problem, you may have been bombarded by confusing terminology and a lot of similar sounding words. Do you have radiculopathy or myelopathy? Your chiropractor said you have a somatic disorder, and your physical therapist called it myofascial pain, and somewhere it showed up on a report as cervicalgia. Could this be neuropathy? Myopathy? |
 |  |
In those cases the spinal cord may be permanently damaged, leaving the patient partially or completely paralyzed (quadriplegic) for life.
What are the symptoms of myelopathy?
They’re a bit different from common neck strains and “pinched nerves”. While radiculopathy causes weakness of one arm (or leg when it happens in the lumbar spine) it also causes severe arm pain, which is the thing that gets most patients off their couch and on the way to the doctor, no matter how nervous that makes them.
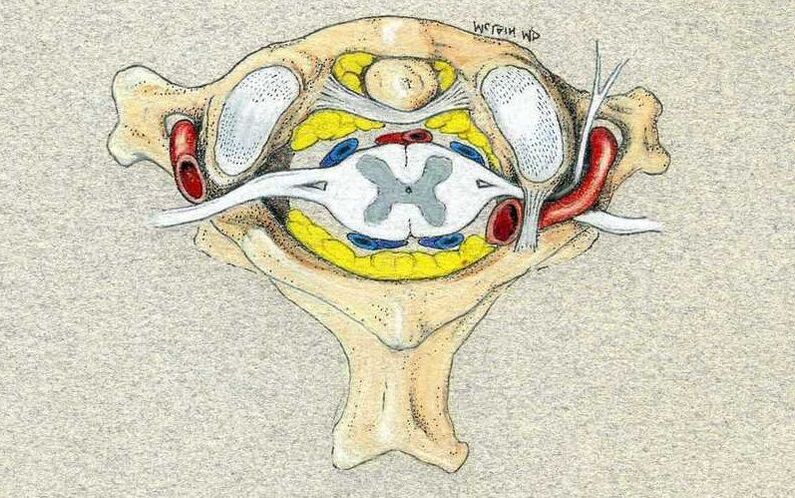
Myelopathy puts pressure on the spinal cord and may not irritate the nerve roots at all. In this case, there may be no severe pain. No arm pain and no new neck pain. Only diminishing function – decreasing strength in both legs. Numbness and tingling in hands and feet, mild at first. Loss of coordination and balance.
What are the symptoms of myelopathy?
They’re a bit different from common neck strains and “pinched nerves”. While radiculopathy causes weakness of one arm (or leg when it happens in the lumbar spine) it also causes severe arm pain, which is the thing that gets most patients off their couch and on the way to the doctor, no matter how nervous that makes them.
Myelopathy puts pressure on the spinal cord and may not irritate the nerve roots at all. In this case, there may be no severe pain. No arm pain and no new neck pain. Only diminishing function – decreasing strength in both legs. Numbness and tingling in hands and feet, mild at first. Loss of coordination and balance.
These symptoms are frequently misdiagnosed by friends and neighbors, spouses and colleagues, and our doctors, as neuropathy (are you diabetic?), arthritis (got bad knees?), old-age (how old were you last year when you didn’t have these symptoms?!?), or more rarely as a serious neurological disorder such as multiple sclerosis or one of its related conditions. In fact, it is fear of the MS diagnosis that sometimes makes patients hesitant to seek a full evaluation.
The symptoms patients may become aware of include neck pain and can include arm pain, but also include spinal cord specific symptoms:
Sometimes the lack of pain creates another problem that patients have a hard time wrapping their head around: “Why do I want to have (a sometimes big) surgery when I’m not having any pain? And HOW, if I have neck pain after surgery, am I any better than I was before surgery?
Reasonable questions.
The best answer is in understanding the goals of treatment. In benign problems like arthritis, and disc herniation, our goal is to relieve pain and restore function. A good result will reduce neck and arm pain and get you back to good function, and any post-operative pain is usually much less than what was going on before surgery. So patients are happy.
- Loss of hand and arm coordination and manual dexterity (can’t button buttons, handwriting is deteriorating)
- Loss of balance and coordination (can’t walk a straight line, can’t walk across the room in the dark)
- Disturbances of bowel and bladder function (incontinence, insensitivity to urination)
- Spasticity (increased reflexes)
- Numbness, tingling, or weakness of both legs or arms ( a pinched nerve affects just one side)
Sometimes the lack of pain creates another problem that patients have a hard time wrapping their head around: “Why do I want to have (a sometimes big) surgery when I’m not having any pain? And HOW, if I have neck pain after surgery, am I any better than I was before surgery?
Reasonable questions.
The best answer is in understanding the goals of treatment. In benign problems like arthritis, and disc herniation, our goal is to relieve pain and restore function. A good result will reduce neck and arm pain and get you back to good function, and any post-operative pain is usually much less than what was going on before surgery. So patients are happy.

With myelopathy, our goal is to take pressure off of the spinal cord and prevent paralysis! That often requires a fairly extensive operation, and there is often a degree of post-operative pain and stiffness that the patient has to work through. And, if all goes well, as it usually does, the biggest bonus is that nothing bad ever happens. Sometimes it’s hard to appreciate that the reward for all this hard work and anxiety is: “I’m not worse!??”
However, worse is sometimes terrible, and your surgeon’s job is to protect you from that in any way possible.
So, what is the treatment for Myelopathy?
The first step is to establish a firm diagnosis. This is actually pretty straight-forward. A typical MRI study will reveal the level and degree of cord compression, if there is any, and will tell us something about the health of the spinal cord itself, providing guidance as to whether this is something we can cautiously plan for, or whether the problem needs to be addressed as an impending emergency.
And the treatment?
Spinal cord compression requires physical decompression. That means surgery is the only way to physically take the pressure off of the cord and restore its normal function.
However, worse is sometimes terrible, and your surgeon’s job is to protect you from that in any way possible.
So, what is the treatment for Myelopathy?
The first step is to establish a firm diagnosis. This is actually pretty straight-forward. A typical MRI study will reveal the level and degree of cord compression, if there is any, and will tell us something about the health of the spinal cord itself, providing guidance as to whether this is something we can cautiously plan for, or whether the problem needs to be addressed as an impending emergency.
And the treatment?
Spinal cord compression requires physical decompression. That means surgery is the only way to physically take the pressure off of the cord and restore its normal function.
Steroids – sometimes wonderful for radicular arm pain – will have no long-term benefit here. Traction, manipulation, physical therapy – can’t change the spinal canal diameter, and can even injure the at-risk spinal cord. Medications may mask some symptoms but won’t change the situation. And this is one of those times when time is not on your side: early treatment is more successful, less risky, and less challenging.
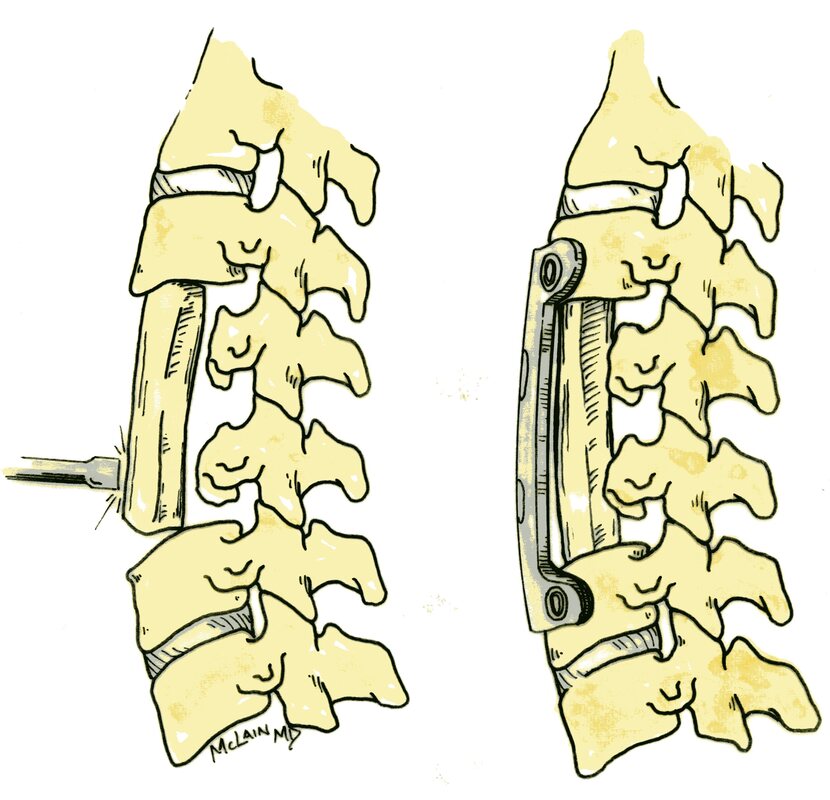
Spinal decompression may be offered through an anterior approach – through the front of the neck – removing herniated discs, disc osteophytes (bone spurs), or entire vertebrae; through a posterior approach (laminectomy) taking the roof off of the spinal canal and decompressing the spinal cord; or frequently may require a combination of the two. These are challenging operations, and almost always require a spinal fusion, immobilization, and post-operative therapy.
If your doctor comes to the conclusion that you have spinal stenosis, or a disc herniation, cervical stenosis, or any other problem causing myelopathy, this is the right time to arrange a consultation with a spine surgeon – even if that’s scary – and not the time to put things off.
The good news is this: with proper treatment spinal cord compression can be relieved - “cured” - and spinal cord function can be preserved and often restored if caught early enough. Post-operative neck pain can be minimized and controlled. And return to normal activities and even sports and recreation are possible.
So, ‘myelopathy’ is that one word (diagnosis) that should catch your doctors eye, and should get you on your way to a specialist evaluation and early treatment without delay. And if you have any of the symptoms I’ve outlined here, don’t hesitate to ask your doctor or therapist directly – “Could this be signs of myelopathy?”
I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share is content with others that might find it beneficial!
Spinal decompression may be offered through an anterior approach – through the front of the neck – removing herniated discs, disc osteophytes (bone spurs), or entire vertebrae; through a posterior approach (laminectomy) taking the roof off of the spinal canal and decompressing the spinal cord; or frequently may require a combination of the two. These are challenging operations, and almost always require a spinal fusion, immobilization, and post-operative therapy.
If your doctor comes to the conclusion that you have spinal stenosis, or a disc herniation, cervical stenosis, or any other problem causing myelopathy, this is the right time to arrange a consultation with a spine surgeon – even if that’s scary – and not the time to put things off.
The good news is this: with proper treatment spinal cord compression can be relieved - “cured” - and spinal cord function can be preserved and often restored if caught early enough. Post-operative neck pain can be minimized and controlled. And return to normal activities and even sports and recreation are possible.
So, ‘myelopathy’ is that one word (diagnosis) that should catch your doctors eye, and should get you on your way to a specialist evaluation and early treatment without delay. And if you have any of the symptoms I’ve outlined here, don’t hesitate to ask your doctor or therapist directly – “Could this be signs of myelopathy?”
I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share is content with others that might find it beneficial!
Whether you are trying to get back into shape, or recovering from an injury, there are some basic exercises you can do to make your back stronger and better able to cope with the rigors of your average day.
When your back hurts it is hard to get moving. Most patients with back pain worry that activity will aggravate their problem, and many fear that it may actually harm them. For the vast majority of patients, nothing could be further from the truth!
Daily activity, and a regular aerobic exercise program, are the keys to getting most people back to good function and are important even in patients that may someday need surgery. Time invested in a physical therapy and exercise program is never wasted.
Daily activity, and a regular aerobic exercise program, are the keys to getting most people back to good function and are important even in patients that may someday need surgery. Time invested in a physical therapy and exercise program is never wasted.

The easiest way to get started with an exercise program is by walking. Walk a bit every day and try and get out at least 3 times a week for a longer walk, and walk quickly for half an hour to 45 minutes. If you're doing it right you should get a little sweaty. Exercise on a treadmill, elliptical trainer, exercise bicycle or in a swimming pool are all good, particularly if the weather outside is nasty.
Patients with narrowing of the spinal canal - spinal stenosis - may find walking difficult. These patients may find an exercise bicycle much easier to exercise on than any upright devices such as a treadmill or elliptical. Patients with disc-related back pain may find sitting on a bicycle difficult, on the other hand, and be more comfortable either swimming or walking.
Find the exercise you can do and do it 3 times a week.
Start with 5-10 minutes of exercise at a time and work up to 30-45 minutes as you are able. Do not get alarmed if you get a little sore after exercising. Keep at it: Moderate exercise will not damage your spine.
Back exercises
Pelvic tilts
Lie down flat on the floor or an exercise pad and bend both knees. Start by tightening your abdominal and buttock muscles. Rotate your pelvis and hips slightly towards the ceiling and press the small of your back against the floor. Hold this position for a moment and then relax.
Patients with narrowing of the spinal canal - spinal stenosis - may find walking difficult. These patients may find an exercise bicycle much easier to exercise on than any upright devices such as a treadmill or elliptical. Patients with disc-related back pain may find sitting on a bicycle difficult, on the other hand, and be more comfortable either swimming or walking.
Find the exercise you can do and do it 3 times a week.
Start with 5-10 minutes of exercise at a time and work up to 30-45 minutes as you are able. Do not get alarmed if you get a little sore after exercising. Keep at it: Moderate exercise will not damage your spine.
Back exercises
Pelvic tilts
Lie down flat on the floor or an exercise pad and bend both knees. Start by tightening your abdominal and buttock muscles. Rotate your pelvis and hips slightly towards the ceiling and press the small of your back against the floor. Hold this position for a moment and then relax.

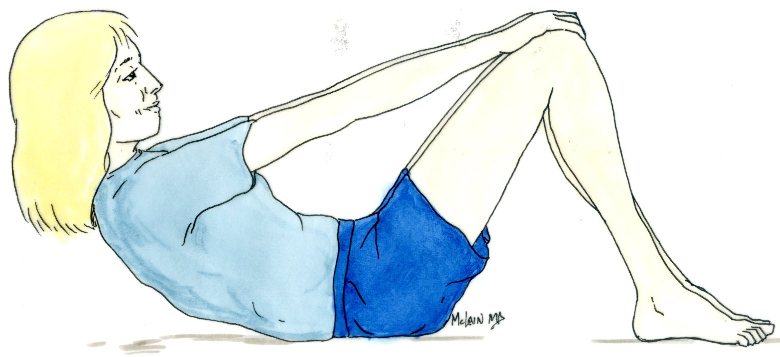
Partial sit up
Laying on your back with both knees bent and your feet flat on the floor, fold your arms across your chest or over your tummy. Tighten your abdominal muscles to raise your chest and shoulders just off the floor.
Don't strain your neck; keep it straight.
Hold your back and shoulder blades off the floor for a count of 3, then relax and let yourself back down. Take a couple of deep breaths, and repeat.
Laying on your back with both knees bent and your feet flat on the floor, fold your arms across your chest or over your tummy. Tighten your abdominal muscles to raise your chest and shoulders just off the floor.
Don't strain your neck; keep it straight.
Hold your back and shoulder blades off the floor for a count of 3, then relax and let yourself back down. Take a couple of deep breaths, and repeat.
Full Sit-ups
For patients with better starting muscles who want to get stronger abdominal wall and pelvic girdle musculature, a full sit-up from the flat position, with the knees bent and the feet anchored, works the deep muscles of the hip flexors as well as the abdominal muscles that help support the spine.
You can do these with your hands reaching for your knees or crossed over your chest. Do three sets of ten – fifteen, and see how your back feels before trying to do more.
Hamstring stretch
Starting flat on your back, with your knees slightly bent, gently flex your hip and bring one of your knees up towards your chest. Holding the knee with your hands, gently pull it towards you until you can feel a stretch. Holding the leg flexed up in that position, straighten the knee out as much as you can, feeling the muscles stretch behind the knee. Lower that leg slowly back to the floor then stretch the other side.
For patients with better starting muscles who want to get stronger abdominal wall and pelvic girdle musculature, a full sit-up from the flat position, with the knees bent and the feet anchored, works the deep muscles of the hip flexors as well as the abdominal muscles that help support the spine.
You can do these with your hands reaching for your knees or crossed over your chest. Do three sets of ten – fifteen, and see how your back feels before trying to do more.
Hamstring stretch
Starting flat on your back, with your knees slightly bent, gently flex your hip and bring one of your knees up towards your chest. Holding the knee with your hands, gently pull it towards you until you can feel a stretch. Holding the leg flexed up in that position, straighten the knee out as much as you can, feeling the muscles stretch behind the knee. Lower that leg slowly back to the floor then stretch the other side.

Wall slide
Find a nice, smooth section of wall, with a stable place to put your feet. Do not try this on a throw rug or something that might slide!
Start with your feet shoulder-width apart, about a foot out from the wall. Lean back until your shoulder blades and buttock are resting comfortably against the wall. Now bend your knees and hips and slowly slide down the wall into a half-sitting position. Pause, then slide back up to your starting position. As you slide, feel your back pressed against the wall. Tightening your abdominal muscles as you move. Your hips should stay higher than your knees, and your knees should not go out beyond your toes.
Find a nice, smooth section of wall, with a stable place to put your feet. Do not try this on a throw rug or something that might slide!
Start with your feet shoulder-width apart, about a foot out from the wall. Lean back until your shoulder blades and buttock are resting comfortably against the wall. Now bend your knees and hips and slowly slide down the wall into a half-sitting position. Pause, then slide back up to your starting position. As you slide, feel your back pressed against the wall. Tightening your abdominal muscles as you move. Your hips should stay higher than your knees, and your knees should not go out beyond your toes.
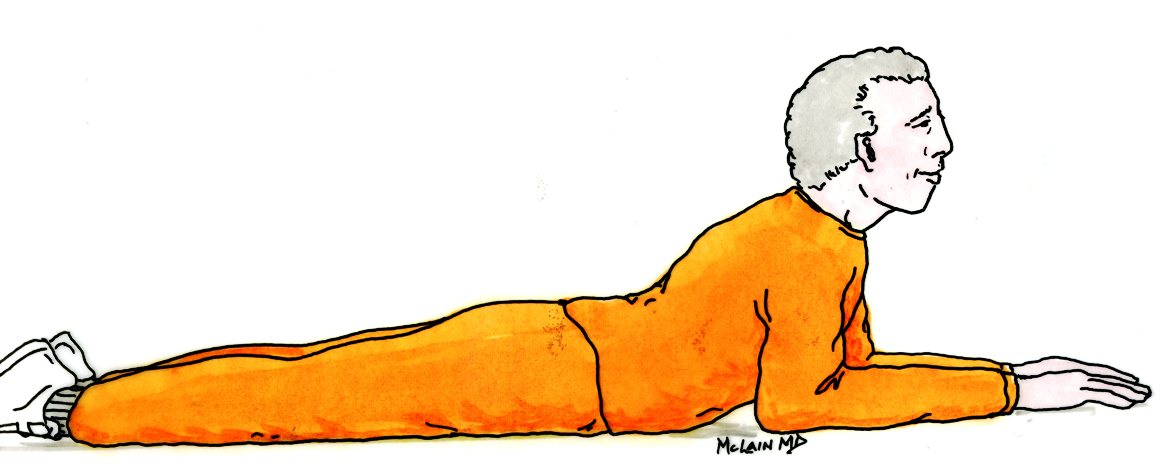
Press ups
Start by lying on your stomach. Put your hands on the floor on either side of your shoulders. Raise your head up and looked towards the far wall.
Straighten your arms and push your upper body up off the floor. Keep your hips in contact with the floor and arch your back. Pause, then slowly bend your elbows and relax your tummy and chest back down to the floor. Don’t go further back than you are comfortable going – this shouldn’t cause sharp pain, so if extension hurts you, you can skip this one.
Arches
Start in the same position that you did with the press ups. This time tuck your arms by your sides, and do not use them to push up. Tightening your back muscles and lift your chest and shoulders up off the floor, again raising your head to look towards the far wall. Hold this position for a count of 5-10, then relax back to your starting position and take a few, well-earned deep breaths.
These exercises will take you 10 – 15 minutes to do each day. Do them each day if you can, but at least four times each week. Do each exercise move 5 times to start, and 10 times each after you get used to it. Move slowly, deliberately, and feel your muscles tighten as you do them. For the Stretches and Press-ups, you should feel stretching, but not sharp pain.
If you feel sore after exercise, that’s normal. Use some ice on the sore-spot, use your anti-inflammatory medications, and go easy the next day. If you experience sharp pain, stop your exercises and note which one seemed to aggravate things. Touch base with your doctor if the pain doesn’t calm down over 48 hours.
I hope you find this program helpful. If you do, feel free to share with others, and let me know if you have other questions I can answer.
Start by lying on your stomach. Put your hands on the floor on either side of your shoulders. Raise your head up and looked towards the far wall.
Straighten your arms and push your upper body up off the floor. Keep your hips in contact with the floor and arch your back. Pause, then slowly bend your elbows and relax your tummy and chest back down to the floor. Don’t go further back than you are comfortable going – this shouldn’t cause sharp pain, so if extension hurts you, you can skip this one.
Arches
Start in the same position that you did with the press ups. This time tuck your arms by your sides, and do not use them to push up. Tightening your back muscles and lift your chest and shoulders up off the floor, again raising your head to look towards the far wall. Hold this position for a count of 5-10, then relax back to your starting position and take a few, well-earned deep breaths.
These exercises will take you 10 – 15 minutes to do each day. Do them each day if you can, but at least four times each week. Do each exercise move 5 times to start, and 10 times each after you get used to it. Move slowly, deliberately, and feel your muscles tighten as you do them. For the Stretches and Press-ups, you should feel stretching, but not sharp pain.
If you feel sore after exercise, that’s normal. Use some ice on the sore-spot, use your anti-inflammatory medications, and go easy the next day. If you experience sharp pain, stop your exercises and note which one seemed to aggravate things. Touch base with your doctor if the pain doesn’t calm down over 48 hours.
I hope you find this program helpful. If you do, feel free to share with others, and let me know if you have other questions I can answer.
Of all the patients that see a spine surgeon, only about 1 in 10 ends up needing to have an operation. No matter how bad your back pain is now, your best bet for improvement in pain and function will include a combination of exercise, conditioning, and improved body mechanics.
Whether you are coping with an acute back injury or long-standing pain, here are some basic recommendations for good health and good spine health, for dealing with pain and starting to get better.
First, start with…
3 things that can help with your overall health:
Weight control and fitness
Controlling your weight and maintaining a good diet will contribute to your overall well-being and will help with reduction of pain in your neck and your lower back. Maintaining a healthy diet, avoiding overeating and snacks, and maintaining a good balance of protein and carbohydrates, will help you heal an injury, and maintain a good healthy fitness level.
Smoking
Cigarette smoking (it’s the nicotine!) is very addictive and it is hard to quit. Nonetheless, stopping smoking can be one of the most important things you can do for the fitness of your spine. Patients with severe back and neck problems really need to stop smoking, as the effect of nicotine on surgical treatment can be very harmful.
Exercise
Diet alone will not keep you from gaining weight, or help you lose it. A good exercise program is always important. Whether or you use an exercise bike, elliptical trainer, treadmill, or swim, walking remains one of the easiest and most effective ways to lose weight and maintain fitness.
3 things that can help with your overall health:
Weight control and fitness
Controlling your weight and maintaining a good diet will contribute to your overall well-being and will help with reduction of pain in your neck and your lower back. Maintaining a healthy diet, avoiding overeating and snacks, and maintaining a good balance of protein and carbohydrates, will help you heal an injury, and maintain a good healthy fitness level.
Smoking
Cigarette smoking (it’s the nicotine!) is very addictive and it is hard to quit. Nonetheless, stopping smoking can be one of the most important things you can do for the fitness of your spine. Patients with severe back and neck problems really need to stop smoking, as the effect of nicotine on surgical treatment can be very harmful.
Exercise
Diet alone will not keep you from gaining weight, or help you lose it. A good exercise program is always important. Whether or you use an exercise bike, elliptical trainer, treadmill, or swim, walking remains one of the easiest and most effective ways to lose weight and maintain fitness.
Now, things you can do to minimize or relieve your back pain:
Good body mechanics
Learning how to sit, stand, and move the right way is important to good back health, and very important to getting over a back injury. Good back and body mechanics reduce the strain on back muscles during normal activities, and help you get back to normal activity without stirring up more pain than you need. Moving the wrong way can be one of the reasons you strained your back in the first place, and it can really slow down your recovery.
Sleeping and laying down
Pain at night can really interfere with rest and recovery. Both leg pain and back pain can be more aggravating at night. If you sleep on your back, put a pillow under your knees, keeping your feet elevated and your hips and knees slightly flexed. When you lay on your side try bending your knees slightly and put a pillow between them to keep your hips even.
Sitting
Make sure your chair supports your back well. Your head should line up over your hips, and you should not feel like you’re slouching. Support your lumbar curve with a rolled-up towel or lumbar roll just behind your back. Your knees should be level with your hips.
Good body mechanics
Learning how to sit, stand, and move the right way is important to good back health, and very important to getting over a back injury. Good back and body mechanics reduce the strain on back muscles during normal activities, and help you get back to normal activity without stirring up more pain than you need. Moving the wrong way can be one of the reasons you strained your back in the first place, and it can really slow down your recovery.
Sleeping and laying down
Pain at night can really interfere with rest and recovery. Both leg pain and back pain can be more aggravating at night. If you sleep on your back, put a pillow under your knees, keeping your feet elevated and your hips and knees slightly flexed. When you lay on your side try bending your knees slightly and put a pillow between them to keep your hips even.
Sitting
Make sure your chair supports your back well. Your head should line up over your hips, and you should not feel like you’re slouching. Support your lumbar curve with a rolled-up towel or lumbar roll just behind your back. Your knees should be level with your hips.

You should take time to change positions and get up and stretch or walk around every half hour or so.
Standing
Standing in one spot is not a mechanical problem for most backs, BUT most of us find ourselves bending forward over our work for long periods of time. Whether you’re doing the dishes, tuning a car, painting a picture or working at a tool bench, that partially flexed position taxes your back muscles and leads to stiffness and pain. Bending your knees slightly will take the stress off your lower back but you can’t stand like that very long. Standing with your foot on a small stool, or even resting it on the floor of an opened cabinet - while working at a counter or sink - will flex your hip, straighten your spine, and take some of the stress of the lumbar musculature.
Remember to wear good quality shoes with a solid arch support. Change positions and move about from time to time.
Bending and lifting
Always use good back mechanics when lifting: Don't cheat! Whether you’re picking up a sock or a rock, bend at your knees and hips instead of your waist. Keep your head and shoulders balanced over your hips and feet.
Lift with your legs, not with your back. Whether you are picking something up off the floor, or a tabletop, or a counter, keep the item close to your body and avoid reaching. And remember, lifting at awkward angles is always a bad idea: Whether you are pulling groceries out of the trunk of your car, or putting your toddler in the car seat, both are much harder on you back than lifting 20 pounds off the top of a counter.
Standing
Standing in one spot is not a mechanical problem for most backs, BUT most of us find ourselves bending forward over our work for long periods of time. Whether you’re doing the dishes, tuning a car, painting a picture or working at a tool bench, that partially flexed position taxes your back muscles and leads to stiffness and pain. Bending your knees slightly will take the stress off your lower back but you can’t stand like that very long. Standing with your foot on a small stool, or even resting it on the floor of an opened cabinet - while working at a counter or sink - will flex your hip, straighten your spine, and take some of the stress of the lumbar musculature.
Remember to wear good quality shoes with a solid arch support. Change positions and move about from time to time.
Bending and lifting
Always use good back mechanics when lifting: Don't cheat! Whether you’re picking up a sock or a rock, bend at your knees and hips instead of your waist. Keep your head and shoulders balanced over your hips and feet.
Lift with your legs, not with your back. Whether you are picking something up off the floor, or a tabletop, or a counter, keep the item close to your body and avoid reaching. And remember, lifting at awkward angles is always a bad idea: Whether you are pulling groceries out of the trunk of your car, or putting your toddler in the car seat, both are much harder on you back than lifting 20 pounds off the top of a counter.
Turning
Learn how to "move as a unit". This means keeping your shoulders and your hips square as you move from place to place. Twisting a little bit to pick something up is not bad, but repetitive twisting back and forth is hard on your back. When you move things from one place to another remember to move your feet as you turn, and not twist at the waist or knees.
Reaching
Good back mechanics means learning how to protect your back whether you are lifting or not. Bending at the waist and leaning forward puts a large strain on back muscles. This is true whether you are tucking sheets on the bed, vacuuming under the couch, getting the milk out of the refrigerator, or lifting something out of your car. Remember to bend your knees, keep your back straight, and work with your legs.
I hope you find this program helpful. If you do, feel free to share with others, and let me know if you have other questions I can answer. Thanks for reading!
Thanks for reading! Feel free to Like and Share this content and let me know what other questions you might have!
Learn how to "move as a unit". This means keeping your shoulders and your hips square as you move from place to place. Twisting a little bit to pick something up is not bad, but repetitive twisting back and forth is hard on your back. When you move things from one place to another remember to move your feet as you turn, and not twist at the waist or knees.
Reaching
Good back mechanics means learning how to protect your back whether you are lifting or not. Bending at the waist and leaning forward puts a large strain on back muscles. This is true whether you are tucking sheets on the bed, vacuuming under the couch, getting the milk out of the refrigerator, or lifting something out of your car. Remember to bend your knees, keep your back straight, and work with your legs.
I hope you find this program helpful. If you do, feel free to share with others, and let me know if you have other questions I can answer. Thanks for reading!
Thanks for reading! Feel free to Like and Share this content and let me know what other questions you might have!
The Opioid Crisis isn’t new. Not hardly. Overuse and abuse of strong pain killers like Percocet or Vicodin has been an issue for back pain and neck pain patients for more than three decades.
But, because of national recognition, legislation, and some high-profile lawsuits, the government – and as a result your pharmacist – have put many changes in place that affect patients with back pain and neck pain who legitimately need those medications.

For doctors treating back and neck pain there is no way around it: while the most satisfying and rewarding part of our job is finding and correcting problems that cause pain, we still have to deal with the actual pain our patients experience before, during, and after surgery or other treatment. As many spine fusion patients can’t take anti-inflammatory medications, we depend on opioid medications to get patients through the first two to four weeks of recovery. That part of post-operative care hasn’t gotten easier as many of the promising “pain killers” of recent years have turned out to be real problems when they get into the wrong hands.
Pharmacies, some of whom have been involved in large lawsuits, have been tasked by law to decide how much medication a patient can have, regardless of what your surgeon or physician has prescribed.
Pharmacies, some of whom have been involved in large lawsuits, have been tasked by law to decide how much medication a patient can have, regardless of what your surgeon or physician has prescribed.
In Ohio pharmacies have adopted the legislated practice of providing no more than a seven day supply of any narcotic/opioid medication, limiting the daily dose, and cannot provide refills. These rules apply to any patient being treated for “acute pain”, whether that acute pain is the result of an ankle sprain or a spinal fusion.
State-wide surveillance systems monitor exactly how much of any “scheduled” medication every patient receives, how often, prescribed by whom, and picked up where. This report is “required reading” literally, for anyone writing you a pain prescription!
There are three things we know about opioid pain medications that can’t be argued: 1. Long-term pain pills are a terrible treatment for ongoing musculoskeletal pain. 2. The longer you take pain pills, the less affective they are, the more pain you feel, and the higher the doses you need to get any relief. 3. After a while, your body will just need the pain pills, whether you have a “pain generator” or not. They are all addicting.
State-wide surveillance systems monitor exactly how much of any “scheduled” medication every patient receives, how often, prescribed by whom, and picked up where. This report is “required reading” literally, for anyone writing you a pain prescription!
There are three things we know about opioid pain medications that can’t be argued: 1. Long-term pain pills are a terrible treatment for ongoing musculoskeletal pain. 2. The longer you take pain pills, the less affective they are, the more pain you feel, and the higher the doses you need to get any relief. 3. After a while, your body will just need the pain pills, whether you have a “pain generator” or not. They are all addicting.
The laws on dispensing opioid medications are pretty hard and fast, and the penalties to your doctor or pharmacist are severe, so there is no wiggle-room here:
How can you avoid getting your pain medication prescriptions all messed up?
Finally, its important to know that – when used appropriately – the most common opioid pain medications are safe and effective. The two most common, hydrocodone (Norco; Vicodin) and oxycodone (Percocet, Roxicet), can be taken over the short-term with little risk of problems. Recent studies have shown that, while these two drugs are the “most commonly abused”, they are also among the “least addictive” of the opioid pain medications we can use for acute pain. The reason they are recognized as being such a problem? – they are far and away the most commonly prescribed and readily available in the community.
That means that – after surgery or a severe injury – you needn’t be afraid of taking prescribed medication to make your pain manageable and make it possible to get up and around and rest comfortably at night. Your pharmacist will make sure you are not getting too much. When your pain calms down, take less. When your pain is tolerable, stop using them altogether. And never share medications with another person, leave your medication where someone else can get at it, or leave it where children or visitors might find it.
Thanks for reading! Feel free to Like and Share this content and let me know what other questions you might have!
How can you avoid getting your pain medication prescriptions all messed up?
- Be straight-forward and open with your pharmacist. Any dishonesty, or perceived dishonesty about what medications you’ve been taking, have recently taken, or what happened to your last prescription will get you “flagged” and your prescription may be denied.
- Even if it’s the perfectly appropriate pain medication, never take medication from someone else’s prescription, or obtain medication in an inappropriate way. This will get you “flagged”.
- Avoid seeking prescriptions from multiple different doctors over a two-year period. After an acute injury and surgery you may have gotten a prescription from your family doctor, another from your Internist, one from the surgical resident, and one from your attending surgeon at the time of discharge – and you are on the borderline. Add one extra trip to the ER and you could be flagged!
- Treat your paper prescription (“script”) like it was an important document – it is! Any evidence that the prescription has been altered – the dosage or number of pills changed, or the signature messed up – may mean the script won’t be accepted. AND – going forward – Ohio pharmacies will no longer be accepting paper scripts except in unique circumstances. Check with your pharmacist before surgery to find out whether an electronic prescription is needed for your post-operative medications.
- Understand that, if your medical or pain specialist doesn’t follow the rules, they can lose their license or worse. If you are already in a pain management program, coordinate your post-operative pain medication management with them. They can provide medication for chronic pain conditions that your surgeon cannot. At the same time, if you pick-up additional prescriptions from your surgeon that they don’t know about it can violate your “contract”. If that happens your source for long-term medication may be dried up, and when you go to any other doctor they will refuse to refill any of what your previous specialist considered legitimate.
Finally, its important to know that – when used appropriately – the most common opioid pain medications are safe and effective. The two most common, hydrocodone (Norco; Vicodin) and oxycodone (Percocet, Roxicet), can be taken over the short-term with little risk of problems. Recent studies have shown that, while these two drugs are the “most commonly abused”, they are also among the “least addictive” of the opioid pain medications we can use for acute pain. The reason they are recognized as being such a problem? – they are far and away the most commonly prescribed and readily available in the community.
That means that – after surgery or a severe injury – you needn’t be afraid of taking prescribed medication to make your pain manageable and make it possible to get up and around and rest comfortably at night. Your pharmacist will make sure you are not getting too much. When your pain calms down, take less. When your pain is tolerable, stop using them altogether. And never share medications with another person, leave your medication where someone else can get at it, or leave it where children or visitors might find it.
Thanks for reading! Feel free to Like and Share this content and let me know what other questions you might have!
I see a number of patients each year who have been treated for chronic leg and back pain with a spinal cord stimulator. For most, it was the last option they had left, and for many it has been a real blessing.
I also see a number of patients each year who have been offered or are considering having a stimulator placed for their ongoing pain. And they usually have a few questions.
Here are a few things you need to know if you are considering a spinal cord stimulator as treatment for your pain:
A spinal cord stimulator (SCS) is a device that generates pulsed electrical signals that directly affect the spinal cord to reduce chronic pain sensations. Similar to deep-brain stimulation, which is now becoming widely used to treat serious motor disorders such as Parkinson disease, the neural stimulators override some signals in the spinal column that are the source of severe and otherwise poorly controlled pain in a variety of disorders.
Here are a few things you need to know if you are considering a spinal cord stimulator as treatment for your pain:
A spinal cord stimulator (SCS) is a device that generates pulsed electrical signals that directly affect the spinal cord to reduce chronic pain sensations. Similar to deep-brain stimulation, which is now becoming widely used to treat serious motor disorders such as Parkinson disease, the neural stimulators override some signals in the spinal column that are the source of severe and otherwise poorly controlled pain in a variety of disorders.

Spinal cord stimulation, in its simplest form, involves the placement of stimulating electrodes or an electrode paddle into the epidural space, inside the spinal canal and on the surface of the spinal cord. This is accompanied by implantation of an electrical pulse generator and battery, usually placed in the lower flank or buttock region, and passage of conducting wires that connect the spinal electrodes to the generator and battery. The generator is then tuned and modulated by remote control once the patient is awake.
Why go through all that?
SCS has notable analgesic properties (it does relieve pain) and, has been proven most effective in treating disorders for which there in no surgical solution or in which additional surgery is out of the question. In my experience, I have seen gratifying results for patients needing management of continued pain from scarring associated with failed back surgery syndrome, from limb pain due to complex regional pain syndrome (RSD), and refractory pain due to ischemic claudication.
Successful outcomes are dependent on careful patient selection, which means your pain doctor has to consider each patient individually and apply very strict “selection criteria” before placement can be approved. For that reason, SCS is not something that your doctor can just put in and turn you loose with.
In my practice, I work with a great group of experienced pain management experts, who see and evaluate each patient, carry out a careful physical and psychological evaluation (that’s absolutely needed before the procedure can be approved, so don’t be alarmed), and carry out a stimulator trial. Those doctors will then determine whether they can convert the stimulator to a permanent unit directly, or whether they need a surgeon to provide the permanent placement. After placement, it’s your pain management doctor, working with the stimulator representative, who can fine tune the system to get you your best result.
Why go through all that?
SCS has notable analgesic properties (it does relieve pain) and, has been proven most effective in treating disorders for which there in no surgical solution or in which additional surgery is out of the question. In my experience, I have seen gratifying results for patients needing management of continued pain from scarring associated with failed back surgery syndrome, from limb pain due to complex regional pain syndrome (RSD), and refractory pain due to ischemic claudication.
Successful outcomes are dependent on careful patient selection, which means your pain doctor has to consider each patient individually and apply very strict “selection criteria” before placement can be approved. For that reason, SCS is not something that your doctor can just put in and turn you loose with.
In my practice, I work with a great group of experienced pain management experts, who see and evaluate each patient, carry out a careful physical and psychological evaluation (that’s absolutely needed before the procedure can be approved, so don’t be alarmed), and carry out a stimulator trial. Those doctors will then determine whether they can convert the stimulator to a permanent unit directly, or whether they need a surgeon to provide the permanent placement. After placement, it’s your pain management doctor, working with the stimulator representative, who can fine tune the system to get you your best result.

Patients typically do best when the majority of their pain involves radicular pain – pain running down the leg or arm - due to nerve hypersensitivity or injury. Patients do best when there is little or no dependence on opioid medications, and when there is minimal psychological overlay (depression, anger, anxiety) associated with their pain. Patients may be screened over a short period with a test or trial lead to determine if the placement provides a proper paresthesia (sensation over the painful area) and to ensure that satisfactory pain relief is achieved.
To be most effective, SCS is provided as a program. No good can be expected from just “having it put in” to see what happens. And the doctor who puts it in needs to be able to manage it or work directly with the experts who performed the trial and can manage the device properly. That’s why I always work hand-in-hand with experienced pain management groups (Cleveland Pain Care) who identify the patients that are likely to do well, do the preoperative testing, and manage the system for best results.
Finally, SCS is not magic, and does not correct the underlying problem that is causing your pain. From time to time I do see a patient who has been offered SCS as the FIRST option in treating their back or radicular leg pain. This is almost never the right way to go, and in each of these cases I’ve discovered clear-cut and sometimes easily correctable causes for pain. That’s an uncommon situation and not something I see among the providers I routinely work with, but it’s something to be aware of.
So, if you find yourself thinking that SCS has been brought up too quickly – or dismissed too quickly – for your pain problem, never hesitate to seek a second opinion.
Thanks for reading. I hope you liked and shared my content. If you have other questions, please comment below.
For more information on Spinal Cord Stimulation, check out (https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/treating-pain-with-spinal-cord-stimulators ) or browse for other links on my website at spinesurgerycleveland.com.
To be most effective, SCS is provided as a program. No good can be expected from just “having it put in” to see what happens. And the doctor who puts it in needs to be able to manage it or work directly with the experts who performed the trial and can manage the device properly. That’s why I always work hand-in-hand with experienced pain management groups (Cleveland Pain Care) who identify the patients that are likely to do well, do the preoperative testing, and manage the system for best results.
Finally, SCS is not magic, and does not correct the underlying problem that is causing your pain. From time to time I do see a patient who has been offered SCS as the FIRST option in treating their back or radicular leg pain. This is almost never the right way to go, and in each of these cases I’ve discovered clear-cut and sometimes easily correctable causes for pain. That’s an uncommon situation and not something I see among the providers I routinely work with, but it’s something to be aware of.
So, if you find yourself thinking that SCS has been brought up too quickly – or dismissed too quickly – for your pain problem, never hesitate to seek a second opinion.
Thanks for reading. I hope you liked and shared my content. If you have other questions, please comment below.
For more information on Spinal Cord Stimulation, check out (https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/treating-pain-with-spinal-cord-stimulators ) or browse for other links on my website at spinesurgerycleveland.com.
Cervical Spine Exercises for preop and post-op patients alike
Any and every patient that comes through my clinic for neck pain or radiculopathy will have some need for an exercise and neck fitness program, if not to avoid cervical spine surgery then to recover from it. It’s universally recognized that an exercise program can reduce neck pain and spasm after an injury as well as surgery can, in most cases, and that after months of pain and limited activity the muscles that support our head and neck weaken and become very susceptible to repeated aggravation and reinjury.
So, a good exercise program is IMPORTANT whether you are avoiding surgery or recovering from it!
Stretching exercises:
It’s usually not necessary to work hard on stretching the neck to regain motion. After an injury or after a bout of muscle spasm, most patients can regain range of motion by working very gently on 3 types of stretching activities:
Gentle stretches: First of all, patients can start by sitting in a common kitchen chair and gently working on relaxation: letting their shoulders relax and letting their neck stretch forward, letting the chin and shoulders fall forward, and relaxing the muscles so that they ease into a slumped posture.
So, a good exercise program is IMPORTANT whether you are avoiding surgery or recovering from it!
Stretching exercises:
It’s usually not necessary to work hard on stretching the neck to regain motion. After an injury or after a bout of muscle spasm, most patients can regain range of motion by working very gently on 3 types of stretching activities:
Gentle stretches: First of all, patients can start by sitting in a common kitchen chair and gently working on relaxation: letting their shoulders relax and letting their neck stretch forward, letting the chin and shoulders fall forward, and relaxing the muscles so that they ease into a slumped posture.
Let this go for 10-20 seconds before sitting upright and stretching the neck back into normal position. Do this a few times until you feel a bit looser.
You can then also stretch your neck backwards by laying flat on your back at the edge of the bed and letting your neck hang over the edge. By gently letting the head roll backwards, you can stretch the muscles in the front of the neck and relieve painful tension.
Finally, while sitting in a chair, you can let your chin fall forward and your head flex forward as far as is comfortable, then gently roll it from side to side, trying to let your ear almost touch your shoulder as you get to each side. You can continue this rotation all the way around the back until you are looking at the ceiling. Then let the spine roll to the other ear and back around in a circle. This gentle range of motion will help stretch all the muscles; it should be done as comfortably as possible with no attempt at actually straining or causing pain. You don't need to push your comfort level.
Isometric strengthening exercises:
Next come the exercises to help restore strength and stamina for the muscles that support your head and neck. Start with this series of gentle isometric exercises that will help strengthen the support muscles of the neck:
These exercises should be done gently to start with and are never intended to involve great strain or produce pain in the neck. If the exercises make you sore, but the soreness is gone by the next day, then you are exercising and working the muscles. If the soreness persists more than a day, however, than you may be overdoing it, and need to back off as the strain may be too much.
Isometric exercises are intended for you to strengthen the muscles without motion of the head or neck. In other words when placing the hand against the side of the head and pressing against a head the hand should not push the head over, nor should the head push the hand away, but both should stay still by pushing against each other equally. This will help the muscle strengthen but won't strain the neck or require great range of motion.
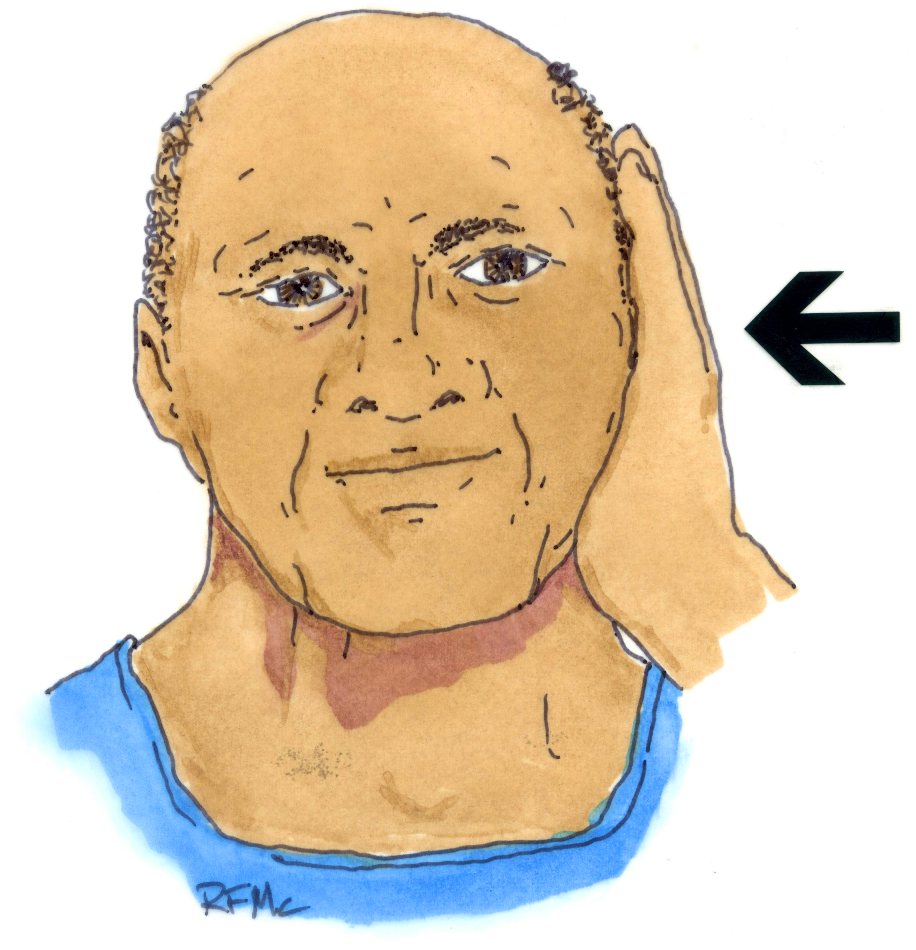
Side bending exercises:
Start off by placing the palm of the hand against the side of your head around the level of the ear or a little higher.
You can then also stretch your neck backwards by laying flat on your back at the edge of the bed and letting your neck hang over the edge. By gently letting the head roll backwards, you can stretch the muscles in the front of the neck and relieve painful tension.
Finally, while sitting in a chair, you can let your chin fall forward and your head flex forward as far as is comfortable, then gently roll it from side to side, trying to let your ear almost touch your shoulder as you get to each side. You can continue this rotation all the way around the back until you are looking at the ceiling. Then let the spine roll to the other ear and back around in a circle. This gentle range of motion will help stretch all the muscles; it should be done as comfortably as possible with no attempt at actually straining or causing pain. You don't need to push your comfort level.
Isometric strengthening exercises:
Next come the exercises to help restore strength and stamina for the muscles that support your head and neck. Start with this series of gentle isometric exercises that will help strengthen the support muscles of the neck:
These exercises should be done gently to start with and are never intended to involve great strain or produce pain in the neck. If the exercises make you sore, but the soreness is gone by the next day, then you are exercising and working the muscles. If the soreness persists more than a day, however, than you may be overdoing it, and need to back off as the strain may be too much.
Isometric exercises are intended for you to strengthen the muscles without motion of the head or neck. In other words when placing the hand against the side of the head and pressing against a head the hand should not push the head over, nor should the head push the hand away, but both should stay still by pushing against each other equally. This will help the muscle strengthen but won't strain the neck or require great range of motion.
Side bending exercises:
Start off by placing the palm of the hand against the side of your head around the level of the ear or a little higher.
Press against the side of your head with the hand, not trying to twist it or bend your neck, and push back against the hand with your head.
You will feel the muscles along the side of your neck and in the front of your neck tighten as you push. Count to 10 than rest and relax. Do this about 5 times to the left-hand side and then 5 times to the right-hand side and then rest and relax. This will help strengthen the muscles both in the front and the back of your neck.
You will feel the muscles along the side of your neck and in the front of your neck tighten as you push. Count to 10 than rest and relax. Do this about 5 times to the left-hand side and then 5 times to the right-hand side and then rest and relax. This will help strengthen the muscles both in the front and the back of your neck.
Forward bending exercise:
Just as you used your hand to press on the side of the head, this exercise simply requires that you push against your forehead with your hand. Pushing back against the forehead as you push forward with your head you'll tighten the muscles in the front of your neck, and you can feel of those tighten along the front of your throat as you push.
Just as you used your hand to press on the side of the head, this exercise simply requires that you push against your forehead with your hand. Pushing back against the forehead as you push forward with your head you'll tighten the muscles in the front of your neck, and you can feel of those tighten along the front of your throat as you push.
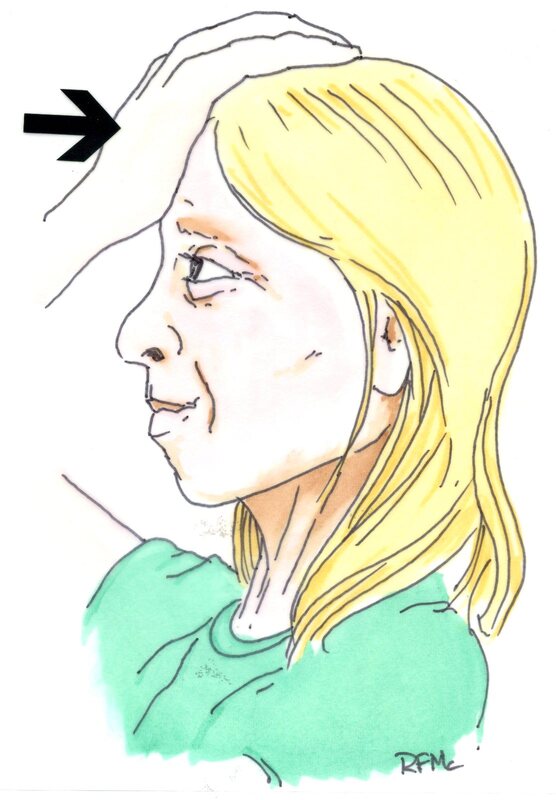
Do this exercise for a count of 10, resting between sets, and do about 5 sets before you quit.
Extension exercises:
Use a small bath towel and place it like a sling behind the back of your head, just at the base of your skull.
Extension exercises:
Use a small bath towel and place it like a sling behind the back of your head, just at the base of your skull.
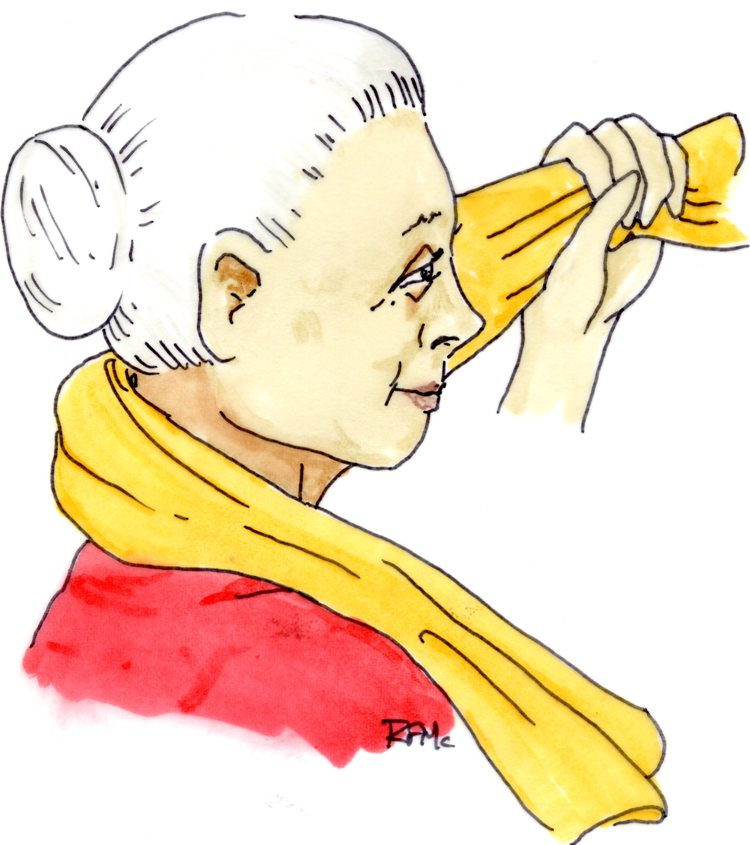 | 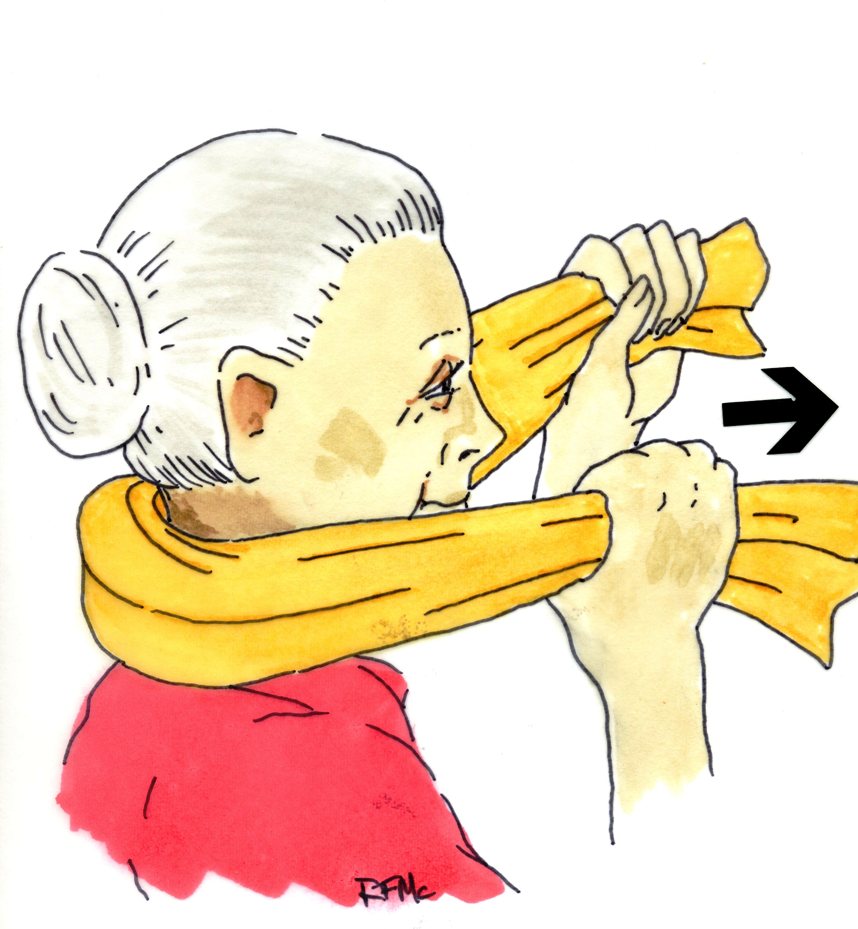 |
Pull the towel up against the back of your head with both hands and pull forward firmly. Push back into the towel with your head so that you do not either bend your head forward or push the towel away.
As you push back into the towel you will feel the muscles on the back of your neck and into your shoulders start to tighten and firm up. This is another exercise that you should do for about 10 seconds at a time using 5 sets as a normal set of exercises. You can do all these exercises while sitting and watching your favorite show, while sitting for lunch, or anytime you have a half-hour to yourself.
Shoulder Girdle exercises:
When you have done your isometric exercises for the neck muscles, you may start doing exercises for the shoulder girdle itself. When we talk about the shoulder girdle, we are talking about the muscles that attach to the neck from the shoulder blades along either side and from the middle of the back. These muscles include the trapezius muscles, the spinal muscles that run right along the spine, and muscles that support the shoulder blade, or scapula, on either side of the neck. Getting these muscles back in shape is often a turning point to overcoming upper back and neck pain and fatigue.
Start by standing upright with your shoulders level and let your shoulders relax at your sides.
Once you have relaxed, with your chin up and neck in neutral position, shrug your shoulders up towards your ears as far as you can, and tighten them and hold them for a count of 10 before resting, letting them come back to their normal position.
As you push back into the towel you will feel the muscles on the back of your neck and into your shoulders start to tighten and firm up. This is another exercise that you should do for about 10 seconds at a time using 5 sets as a normal set of exercises. You can do all these exercises while sitting and watching your favorite show, while sitting for lunch, or anytime you have a half-hour to yourself.
Shoulder Girdle exercises:
When you have done your isometric exercises for the neck muscles, you may start doing exercises for the shoulder girdle itself. When we talk about the shoulder girdle, we are talking about the muscles that attach to the neck from the shoulder blades along either side and from the middle of the back. These muscles include the trapezius muscles, the spinal muscles that run right along the spine, and muscles that support the shoulder blade, or scapula, on either side of the neck. Getting these muscles back in shape is often a turning point to overcoming upper back and neck pain and fatigue.
Start by standing upright with your shoulders level and let your shoulders relax at your sides.
Once you have relaxed, with your chin up and neck in neutral position, shrug your shoulders up towards your ears as far as you can, and tighten them and hold them for a count of 10 before resting, letting them come back to their normal position.
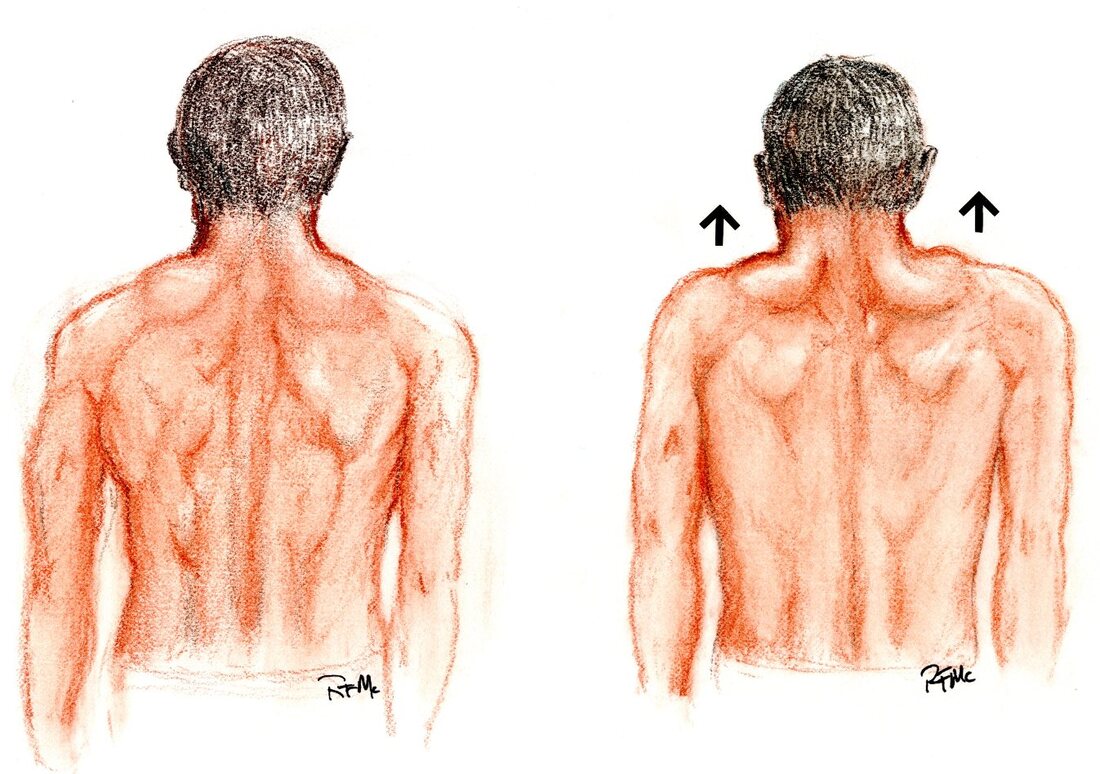
You can do this exercise while holding weights in your hand, but I would start with no more than 5 pounds in the hands and work up gradually with weights if you want to. As you get comfortable with this you can add more repetitions and perform the shoulder shrugs as you rotate your shoulders – still with your arms at the sides - from front to back, ten times.
A final exercise that will help build the shoulders up is to squeeze the shoulder blades together as though you were trying to pinch a piece of paper between the shoulder blades behind your back.
A final exercise that will help build the shoulders up is to squeeze the shoulder blades together as though you were trying to pinch a piece of paper between the shoulder blades behind your back.
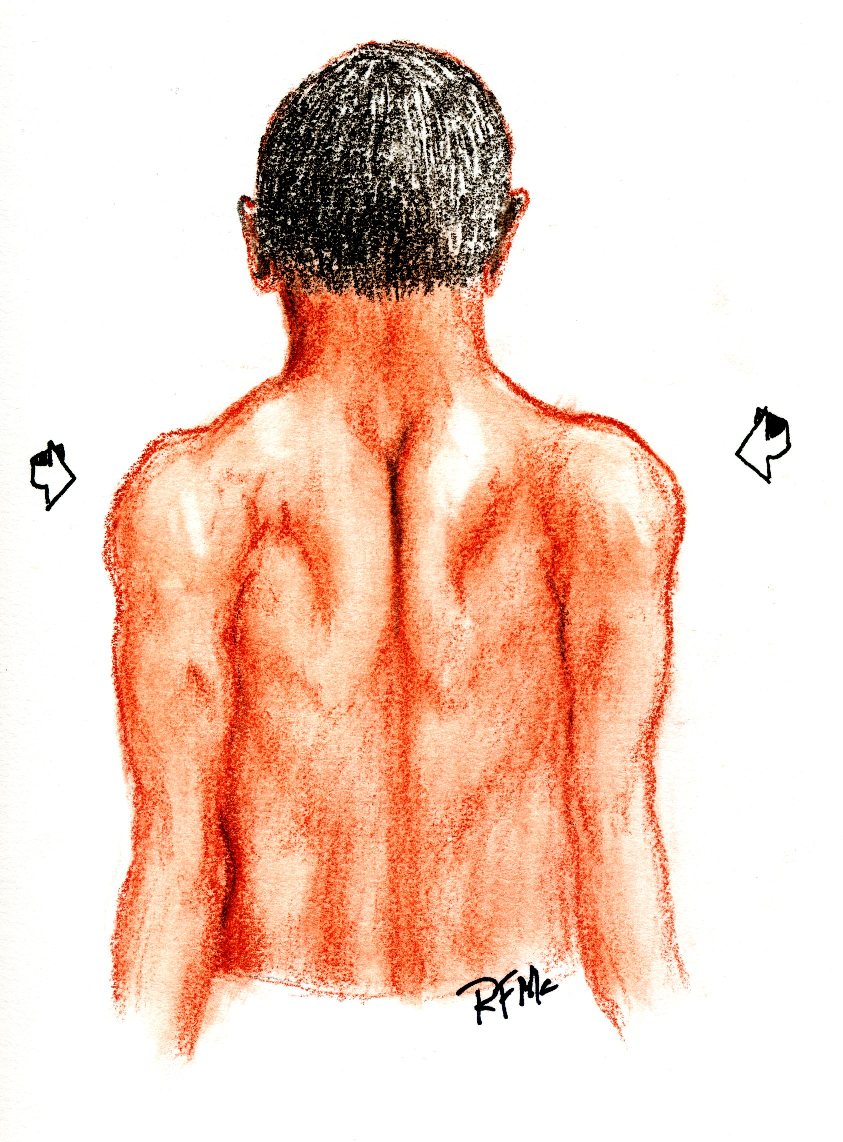
Squeeze the shoulder blades together and hold on there for a count of 10 then rest and relax.
Hopefully these exercises will get you back to better neck motion, better activity, and restful sleep. Give any physical therapy program time to work – results can be seen after 6 – 8 weeks of exercise, but not after 6 – 8 days, so don’t get discouraged. And remember to use your anti-inflammatory medications, and ice and heat as needed, to help with soreness and stiffness.
For more information on neck pain, cervical disc disease, and the surgeries that can treat them, browse for other links on my website at spinesurgerycleveland.com.
I hope you found this information useful. If you did, consider liking and sharing with others. Thanks for reading!
Hopefully these exercises will get you back to better neck motion, better activity, and restful sleep. Give any physical therapy program time to work – results can be seen after 6 – 8 weeks of exercise, but not after 6 – 8 days, so don’t get discouraged. And remember to use your anti-inflammatory medications, and ice and heat as needed, to help with soreness and stiffness.
For more information on neck pain, cervical disc disease, and the surgeries that can treat them, browse for other links on my website at spinesurgerycleveland.com.
I hope you found this information useful. If you did, consider liking and sharing with others. Thanks for reading!
Author
I'm Dr. Rob McLain. I've been taking care of back and neck pain patients for more than 30 years. I'm a spine surgeon. But one of my most important jobs is...
answering questions!
Archives
January 2024
May 2023
February 2023
January 2023
December 2022
November 2022
October 2022
September 2022
August 2022
July 2022
 RSS Feed
RSS Feed