If you’ve been to more than one doctor for a neck pain problem, you may have been bombarded by confusing terminology and a lot of similar sounding words. Do you have radiculopathy or myelopathy? Your chiropractor said you have a somatic disorder, and your physical therapist called it myofascial pain, and somewhere it showed up on a report as cervicalgia. Could this be neuropathy? Myopathy? |
 |  |
In those cases the spinal cord may be permanently damaged, leaving the patient partially or completely paralyzed (quadriplegic) for life.
What are the symptoms of myelopathy?
They’re a bit different from common neck strains and “pinched nerves”. While radiculopathy causes weakness of one arm (or leg when it happens in the lumbar spine) it also causes severe arm pain, which is the thing that gets most patients off their couch and on the way to the doctor, no matter how nervous that makes them.
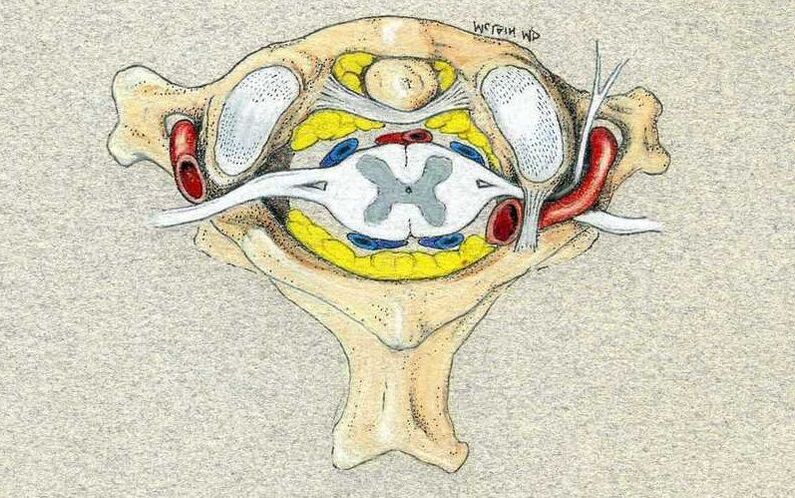
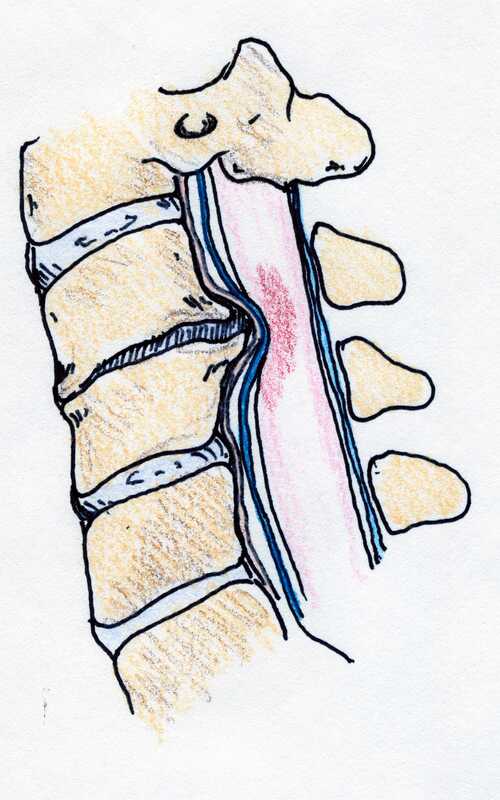
Myelopathy puts pressure on the spinal cord and may not irritate the nerve roots at all. In this case, there may be no severe pain. No arm pain and no new neck pain. Only diminishing function – decreasing strength in both legs. Numbness and tingling in hands and feet, mild at first. Loss of coordination and balance.
What are the symptoms of myelopathy?
They’re a bit different from common neck strains and “pinched nerves”. While radiculopathy causes weakness of one arm (or leg when it happens in the lumbar spine) it also causes severe arm pain, which is the thing that gets most patients off their couch and on the way to the doctor, no matter how nervous that makes them.
Myelopathy puts pressure on the spinal cord and may not irritate the nerve roots at all. In this case, there may be no severe pain. No arm pain and no new neck pain. Only diminishing function – decreasing strength in both legs. Numbness and tingling in hands and feet, mild at first. Loss of coordination and balance.
These symptoms are frequently misdiagnosed by friends and neighbors, spouses and colleagues, and our doctors, as neuropathy (are you diabetic?), arthritis (got bad knees?), old-age (how old were you last year when you didn’t have these symptoms?!?), or more rarely as a serious neurological disorder such as multiple sclerosis or one of its related conditions. In fact, it is fear of the MS diagnosis that sometimes makes patients hesitant to seek a full evaluation.
The symptoms patients may become aware of include neck pain and can include arm pain, but also include spinal cord specific symptoms:
Sometimes the lack of pain creates another problem that patients have a hard time wrapping their head around: “Why do I want to have (a sometimes big) surgery when I’m not having any pain? And HOW, if I have neck pain after surgery, am I any better than I was before surgery?
Reasonable questions.
The best answer is in understanding the goals of treatment. In benign problems like arthritis, and disc herniation, our goal is to relieve pain and restore function. A good result will reduce neck and arm pain and get you back to good function, and any post-operative pain is usually much less than what was going on before surgery. So patients are happy.
- Loss of hand and arm coordination and manual dexterity (can’t button buttons, handwriting is deteriorating)
- Loss of balance and coordination (can’t walk a straight line, can’t walk across the room in the dark)
- Disturbances of bowel and bladder function (incontinence, insensitivity to urination)
- Spasticity (increased reflexes)
- Numbness, tingling, or weakness of both legs or arms ( a pinched nerve affects just one side)
Sometimes the lack of pain creates another problem that patients have a hard time wrapping their head around: “Why do I want to have (a sometimes big) surgery when I’m not having any pain? And HOW, if I have neck pain after surgery, am I any better than I was before surgery?
Reasonable questions.
The best answer is in understanding the goals of treatment. In benign problems like arthritis, and disc herniation, our goal is to relieve pain and restore function. A good result will reduce neck and arm pain and get you back to good function, and any post-operative pain is usually much less than what was going on before surgery. So patients are happy.

With myelopathy, our goal is to take pressure off of the spinal cord and prevent paralysis! That often requires a fairly extensive operation, and there is often a degree of post-operative pain and stiffness that the patient has to work through. And, if all goes well, as it usually does, the biggest bonus is that nothing bad ever happens. Sometimes it’s hard to appreciate that the reward for all this hard work and anxiety is: “I’m not worse!??”
However, worse is sometimes terrible, and your surgeon’s job is to protect you from that in any way possible.
So, what is the treatment for Myelopathy?
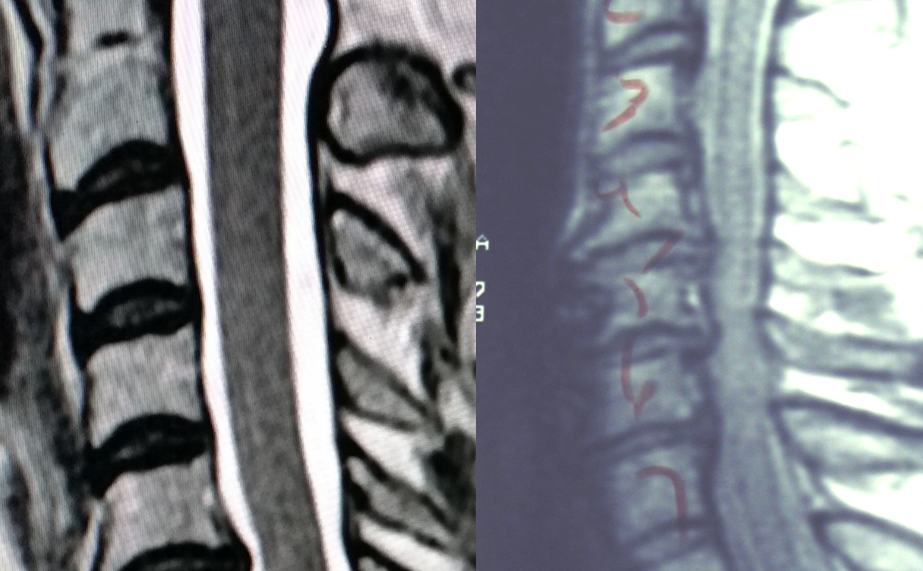
The first step is to establish a firm diagnosis. This is actually pretty straight-forward. A typical MRI study will reveal the level and degree of cord compression, if there is any, and will tell us something about the health of the spinal cord itself, providing guidance as to whether this is something we can cautiously plan for, or whether the problem needs to be addressed as an impending emergency.
And the treatment?
Spinal cord compression requires physical decompression. That means surgery is the only way to physically take the pressure off of the cord and restore its normal function.
However, worse is sometimes terrible, and your surgeon’s job is to protect you from that in any way possible.
So, what is the treatment for Myelopathy?
The first step is to establish a firm diagnosis. This is actually pretty straight-forward. A typical MRI study will reveal the level and degree of cord compression, if there is any, and will tell us something about the health of the spinal cord itself, providing guidance as to whether this is something we can cautiously plan for, or whether the problem needs to be addressed as an impending emergency.
And the treatment?
Spinal cord compression requires physical decompression. That means surgery is the only way to physically take the pressure off of the cord and restore its normal function.
Steroids – sometimes wonderful for radicular arm pain – will have no long-term benefit here. Traction, manipulation, physical therapy – can’t change the spinal canal diameter, and can even injure the at-risk spinal cord. Medications may mask some symptoms but won’t change the situation. And this is one of those times when time is not on your side: early treatment is more successful, less risky, and less challenging.
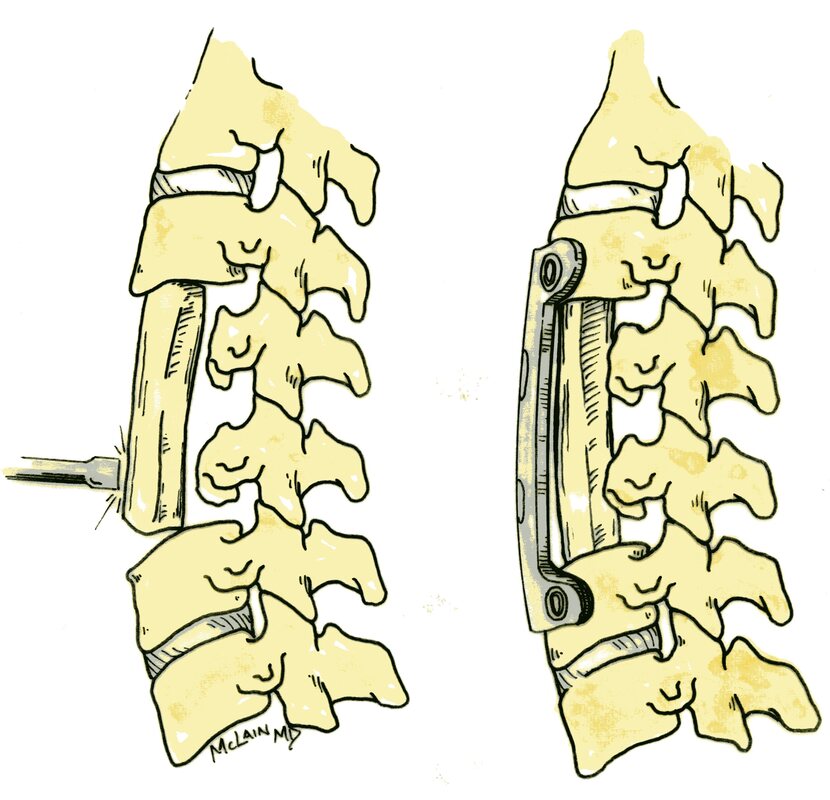
Spinal decompression may be offered through an anterior approach – through the front of the neck – removing herniated discs, disc osteophytes (bone spurs), or entire vertebrae; through a posterior approach (laminectomy) taking the roof off of the spinal canal and decompressing the spinal cord; or frequently may require a combination of the two. These are challenging operations, and almost always require a spinal fusion, immobilization, and post-operative therapy.
If your doctor comes to the conclusion that you have spinal stenosis, or a disc herniation, cervical stenosis, or any other problem causing myelopathy, this is the right time to arrange a consultation with a spine surgeon – even if that’s scary – and not the time to put things off.
The good news is this: with proper treatment spinal cord compression can be relieved - “cured” - and spinal cord function can be preserved and often restored if caught early enough. Post-operative neck pain can be minimized and controlled. And return to normal activities and even sports and recreation are possible.
So, ‘myelopathy’ is that one word (diagnosis) that should catch your doctors eye, and should get you on your way to a specialist evaluation and early treatment without delay. And if you have any of the symptoms I’ve outlined here, don’t hesitate to ask your doctor or therapist directly – “Could this be signs of myelopathy?”
I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share is content with others that might find it beneficial!
Spinal decompression may be offered through an anterior approach – through the front of the neck – removing herniated discs, disc osteophytes (bone spurs), or entire vertebrae; through a posterior approach (laminectomy) taking the roof off of the spinal canal and decompressing the spinal cord; or frequently may require a combination of the two. These are challenging operations, and almost always require a spinal fusion, immobilization, and post-operative therapy.
If your doctor comes to the conclusion that you have spinal stenosis, or a disc herniation, cervical stenosis, or any other problem causing myelopathy, this is the right time to arrange a consultation with a spine surgeon – even if that’s scary – and not the time to put things off.
The good news is this: with proper treatment spinal cord compression can be relieved - “cured” - and spinal cord function can be preserved and often restored if caught early enough. Post-operative neck pain can be minimized and controlled. And return to normal activities and even sports and recreation are possible.
So, ‘myelopathy’ is that one word (diagnosis) that should catch your doctors eye, and should get you on your way to a specialist evaluation and early treatment without delay. And if you have any of the symptoms I’ve outlined here, don’t hesitate to ask your doctor or therapist directly – “Could this be signs of myelopathy?”
I hope you find this discussion interesting and useful. If you have other questions that I can answer for you, please comment below. And feel free to like and share is content with others that might find it beneficial!
0 Comments
Leave a Reply.
Author
I'm Dr. Rob McLain. I've been taking care of back and neck pain patients for more than 30 years. I'm a spine surgeon. But one of my most important jobs is...
answering questions!
Archives
January 2024
May 2023
February 2023
January 2023
December 2022
November 2022
October 2022
September 2022
August 2022
July 2022
 RSS Feed
RSS Feed